It was around the year 1590 when mankind figured out how to use optical lenses to bring into sight things smaller than the natural eye can observe. With the invention of the microscope, a new and unexplored world was discovered. It will likely be of great surprise to the reader that scientists of the time did not believe that within this new microscopic realm lay the source of sickness and disease. Most would still hold on to a belief of what was known as Miasma theory, which dates back to the Roman Empire. This theory states that the source of disease was contaminated air through decomposing organic materials. It wouldn’t be until the 1850’s that a man by the name of Louis Pasteur, from whom we get “pasteurization”, would promote Germ Theory into the spotlight of the sciences.
Pasteur, considered by many as the father of microbiology, would go on to assist fellow biologist Charles Chameberland in the invention of the aptly named Pasteur Chamberland filter — a porcelain filter with a pore size between 100 and 1000 nanometers. This was small enough to filter out the microscopic bacteria and cells known at that time from a liquid suspension, leaving behind a supply of uncontaminated water. But like so many other early scientific instrumentation inventions it would lead to the discovery of something unexpected. In this case, a world far smaller than 100 nanometers… and add yet another dimension to the ever-shrinking world of the microscopic.
This is when we began to learn about viruses.
Discovery of the Virus and the Vaccine
The word “virus” stems from the Latin phrase “slimy fluid“. In 1898, a man by the name of Martinus Beijerinck passed a solution containing a still unknown infectious agent that targeted tobacco plants through a Pasteur Chamberland filter. The purified solution was applied to a healthy tobacco plant and to his great surprise the plant became infected. He concluded that the infectious agent was unfilterable, and took an even further leap to describe the infectious agent as a “living liquid”.
In that same year, a pair of German scientists, Friedrich Loeffler and Paul Frosch, performed the same experiment which returned the same results with what we now know as Foot-and-Mouth Disease (FMDV) in livestock. They, however, did not agree with Beijerinck’s conclusion of the infectious agent being a living liquid. But instead believed it to be a particulate that was smaller than the porcelain filter pore size. They pushed forward with their belief by heating the filter element to “destroy the agent’s infectivity”, though it was not clear to them as to how heat destroyed it. Nevertheless, they were successful in creating an FMDV vaccine for cows and sheep from the infectious solution that was passed through the heated filter, which put more precedence on understanding a virus as an ultrascopic living particulate, and not a living liquid.
It should be noted that the smallpox vaccine was widely used at this time, though no one had any understanding of how it worked or what it even was. Indeed, the term vaccine is derived from the Latin word vacca, which translates directly to cow. This odd relationship owes its history to the somewhat accidental discovery that milkmaids who often contracted a very mild disease called cowpox did not get infected with the much more severe smallpox disease. In 1796, a cruel experiment was performed by a man named Edward Jenner. He took puss from a cowpox blister and purposely infected a young boy. Once the boy recovered, he repeated the process with smallpox and found that the boy did not get the disease. Jenner’s vaccination technique would not only go on to save millions of lives from smallpox; it would be used to vaccinate people from several other diseases, including polio and yellow fever.
The Birth of Molecular Biology
The next few decades would identify hundreds of viruses of all shapes and sizes, and along with them various types of vaccines. But it was the study of exactly what these viruses were and how the vaccines actually worked that would give rise to a revolutionary new science — molecular biology.
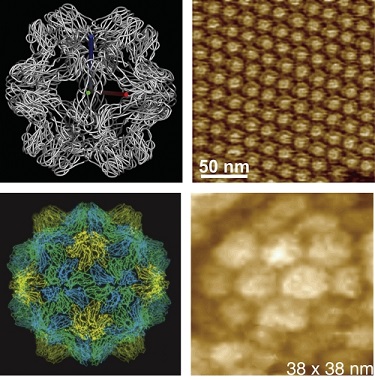
New technologies such as electron microscopy, along with other advances in scientific understandings would show that viruses are some of the smallest lifeforms on earth. It could even be argued that they’re not alive at all… an debate that carries on to this day. Our own [Dan Maloney] has written several articles on the details of how viruses and our immune system work at a molecular level. And the clever ways we try to stop viruses. However, there is still much to be learned.
Understanding viruses at the molecular level presents a very real modern day challenge. Despite the full power, wealth, and knowledge of our modern civilization, a tiny packet of RNA enclosed in a fatty drop continues to wreak havoc on our world. The COVID-19 virus has in some shape, form, or fashion effected every single human being on earth. Those viruses once invisible to us now stand before our very eyes in full view, and yet we have suffered terrible losses to this one. Our best tool is a breakthrough barely 30 years old — our ability to tailor messenger RNA (mRNA) a targeted purpose — has very quickly led to a viable vaccine. There is no doubt in my mind that eventually this virus will succumb to the might of human ingenuity that has been unlocked by more than a century of cumulative scientific knowledge.














Tah, FWIW I understand seawater has some 25 billion phage viruii per litre ie Almost all are bacterial viruses, hence why dipping infected body parts in seawater can (sometimes depending on condition) alleviate many wound bacterial infections…
I don’t believe the second aspect is particularly true i.e. what is holding back phage therapy is it’s hard to produce an effective phage treatment for bacterial infections.
Like most viruses phages can be exceptionally restricted in which cells they can infect.
COVID-19 not withstanding successful/virulent species jumping is rare among viruses and unfortunately there is not much call for super syphilis in the ocean to maintain a population of phages which infect syphilis to treat a person.
So why does sea water help wounds? Mostly just for cleaning. The story comes from burns injurys (WWII pilots) who were sea water protected the wound compared to being burning and in a dry place…
That said phage therpay is very exciting it’s just dip your ingrown toe nail in the sea is the equivalent to here rub this bbq coal on your face activated charcoal is purifying!
Pfft – good to read more widely, I’m fortunate in my case with benefit of post grad 2010 in food science where bacteriology and viruii given broad attention, have moved on from there. Phage therapy in general rather difficult – Many permutations and also not pursued that much due to advances in antibiotics in a pharmaceutical competitive environment which projects a form of prejudice protecting their income displacing drive for pertinent research.
Helpful to read more before making claims on beliefs Alex Rossie, here’s a link re phage & their staggering numbers. The references of course the more useful regions in Wikipedia, a very complex field replete with experiences of decades across the globe.
https://en.wikipedia.org/wiki/Bacteriophage
Seawater appears much more variable in modern industrial times, Eg I wouldn’t put my body in the waters off global industrial regions rich in mercury and lead these days if I had a persistent antibiotic resistant infection. Lots of historic ancedotal evidence and in early pre advanced antibiotic times too of studies into value of seawater around the world especially third world countries and estuaries discharging mineral rich waters from volcanic regions ie high in copper, zinc mixing with sea iodine, viruii entrapment in seaweeds eyc. So it’s not just the immense variants of phage but also minerals enhancing recuperative experiences by way of mRNA metabolizing various differences in enzymes eg SOD1 (high Cu/An) variants and others outside our comparatively narrow adapted human immune system. The paradigm is complex and frowned upon by many in the medical industry marketed to by big pharma.
Antibiotics of course for sheer efficiency and efficacy have their place as a first direct line of defence but, nature offers millenia of adaptations offering immense permutations. The very wide bell curve of phage types not to be discounted and thus inappropriate to project any idea dissuading of those with a persistent bacterial infection considered slow to respond to (expensive) antibiotics.
Go for a long swim, enjoy yourself and let those trillions of phage too swarm around as you dog paddle and they do their thing. Since our human cells immune to the phage variants it’s borderline an imperative we adapted to that environment for millennia unlike other primates, ie we evolved in close proximity to the seas, evidence from downward facing nose, hair swirls, baby diving and innate swimming response etc…
You’re talking nonsense here.
Bacteriophages are sometimes specific down to the substrain of species they infect.
The stories of healing pools related to feaco-oral infections where the causative bacteria thrived in the water source where the phages lived. And still these were not of practical use.
On the other hand in the treatment of respiratory infections is where phage therapy shines (actually pseudomonas respiratory infections are the most promising avenue for phage therapy), don’t have a closed pool where phages can evolve to infect them. They evolved in hospital settings in a pool of a cocktail of antibiotics. They are dramatically different from the pseudomonas you will find outside of a CF patients lungs or clinic.
So jumping into the ocean will not treat any condition effectively (beyond the effects of saline). It is precisely because the bacteria that infect skin are so different from the bateria that live in sea water that there is any benefit to being in sea water (e.g. the WWII pilots I described above).
I will not be continuing this conversation as there is far too much risk of disinformation which you seem only too happy to spew.
Here is a brief summary of just why you’re talking nonsense https://www.ncbi.nlm.nih.gov/books/NBK493185/
I can personally attest to this myself. I’ve had a fungal infection on my skin which simply wouldn’t go away with whatever creams I would put on it, though in retrospect I probably wasn’t applying it properly. I went for a swim in the sea and it somehow magically disappeared. I think it also happened a second time to me as well, but I cant remmeber the details.
Of course it’s all anecdotal. And the infection was fungal, not bacterial (according to my doctor anyway). I don’t know if phages work on fungi, or if it was phages that did the work (it could’ve been just the salt), but I do think seawater can do some magic on the skin and certain diseases.
I didn’t see any mention in this article of Antoine Bechamp. A history of germ theory is hardly complete without at least a mention of him. Is anyone here familiar?
“This theory states that the source of disease was contaminated air through decomposing organic materials”
Which is actually a pretty good guess given the circumstances. They figured out the parts they could observe and drew incorrect but feasible conclusions. No mystical mumbo-jumbo but science!
I suppose for all that man kind missed out on before the microscope at seeing the wonders of the microcosm they gained by having unpolluted view of the macrocosm!
I still wonder what our next major discovery will be, everyone is keyed onto space travel which is of course exciting. But I’m more excited about what I can’t see on the horizon.
The thing that consistently blows me away is how compact viruses are in terms of data. COVID-19 is just under 8KB of data at two bits per base pair… What other 8k message would cause so much chaos on earth?
SQL Slammer was only 404 bytes.
That is an interesting observation drenehestral. I think it is even more unsettling than the fact that our human DNA code could fit on a single CD (700MB)
“Why It Actually Took 50 Years to Make COVID mRNA Vaccines”
https://youtu.be/XPeeCyJReZw
You’d figure they would have found a less invasive way to test, in all that time. It’s still the long Q-tip, way up the nose. I would have also thought there would have been a better delivery system, than shoving a hunk of metal deep into muscle tissue. Probably almost never happens, but there are arteries, nerves, and a few other things, getting nicked, or pierced by the needle. Small needle, small damage, but I think it can do enough to mess you up for a few days.
Vaccines are typically delivered by injection into muscle tissue, and the easiest way to do so remains the needle.
We’re really great at vaccinating thesedays, well done to the Pfizer, Oxford and every other vaccine development team around the world. But why in 2020 did we forget the basic principles of good hygiene, as emphasized at:
http://www.upmc-biosecurity.org/website/resources/publications/2006/2006-09-15-diseasemitigationcontrolpandemicflu.html
“In 1796 …a man named Edward Jenner”… in 1796 the method was already known to Europe, China, India, Africa… ( https://en.wikipedia.org/wiki/Inoculation#Origins ).
I think this
https://www.researchgate.net/publication/6563882_Disease_Mitigation_Measures_in_the_Control_of_Pandemic_Influenza
could make a really good addition to this page. Alongside the wonder of vaccination, probably the most effective single medical breakthrough ever, there is also the matetr of how to control disease in the effective and precedented way in that irritating period before you’ve rolled the vaccine(s) out widely ernough. This paper address it really well. The last author on it is the guy who eradicated smallpox, I can’t think of a better expert on the subject matter.
Good to see, fwiw in our early human periods pre Bessemer steel process and before electrical industry, many ate from copper bowls ingesting high levels by virtue of food acids. Our prime immune enzyme SOD1 requires healthy copper levels for optimum function plus the other 140+ copper enzymes incl metabolizing iron re anemia. Most on planet unfortunately very deficient in copper Eg old nutritional suggestions of 1mg/day intrinsically false, more recent tissue culture and related exposure studies show homeostasis level 0.1mg/Kg body/day with many western diet regions offering as little as 0.5mg per day ie Serious deficiency. The only contraindication via the genetic Wilson’s disease also not well understood and rare with lots of propaganda re copper and vague ideas of toxicity markers, ie false.
Most troubling as our brain has highest concentration of copper over all organs incl liver eg NMDA receptor dependent upon it And related to cognitive functionality incl prions and memory types eg intellectual vs emotional primal (tribal) response patterns, eg polarisation ;-)
In any case, this populist link likely more pertinent to the general audience type in careers outside biochemistry:-
https://mobile.twitter.com/ajenglish/status/1363684941788250118?s=25
Go and look up “Variolation” as used in China as early as the fifteenth century. Interestingly they selected mild case as the donors and denatured the sample by drying it.
“Those viruses once invisible to us now stand before our very eyes in full view, and yet we have suffered terrible losses to this one”
Yes – if you are referring to financial losses. The loss of life (considering the term “pandemic”) is minimal, compared to other pandemics such as the “Great Plagues”, smallpox, cholera, etc. I mean Covid, even if left unchecked wouldn’t hold a candle to those. to be fair, this is the “best” pandemic scenario one can hope for. It’s best to not have a pandemic at all. But I have to have one, Covid-19 is my choice :)
I need someone to explain why no one is talking about the fact that SARS-COV and SARS-COV2 had already been documented prior to the outbreak. The notes from the swabs taken from the bats in china were posted online. There has also been zero communication in the media about the fact you can be infected via the skin and eyes and that masks cannot filter reliably below 300-500 microns. This had already been tested in a live environment, in hospitals and on planes with live virii.
The virus virion size is never mentioned but you can dig through documentation stating its 40-70nm average size with a max of 120nm. What does that mean once there are hundreds of thousands of particles floating around in an Hospital whose HVAC couldn’t even handle Ebola prior to 2019. In 2003 we knew of asymptomatic spread, spread via the wind and aerosols, that animals and bugs could be carriers and that it SARS could be tracked via the sewers, and that the testing was not reliable. This info is all available via the CDC and CIDRAP web sites since 2003 yet the rest of the world went on as if this had not already happened back in 2002. We also knew that the vaccine that was being worked on didn’t create antibodies that lasted past 30-90 days.
Nobody is mentioning the missing recordings and interviews from the CDC either or the fact that the WHO did not have any virus samples from Chinese patients. Not one sample and didn’t know when they would get a sample either. The man that warned us about the outbreak never provided samples either because he died and nobody from the WHO or CDC went there to get samples either. Now the CDC is acting like there was nothing going on when IHR2005 protocol was not being followed. The Chinese signed IHR2005. They were obligated to provide samples and chose not to in November.
Not one mention of the Canadian investigation into the 2002 outbreak either.
Why?
9/10. Great effort, amazing content.
For the final 1/10 the sentence “It could even be argued that they’re not alive at all… an debate that…” needs to be corrected.
It’s “a debate” not “an debate”.